https://drive.google.com/a/bu.
Friday, May 9, 2014
Final Presentation Done!
We finally finished our final presentation for the class.
https://drive.google.com/a/bu.
https://drive.google.com/a/bu.
Saturday, May 3, 2014
Final Project Presentation Video Made
We finally made a demo video of our product. I edited the videos and uploaded it to youtube.
Monday, April 28, 2014
Final Project Design Tasks
Now that we are in the last week of classes, we need to buckle down and figure out how to demonstrate our final design. The major change/addition we will have for the final presentation is the microneedle array. We have decided that the best way to demonstrate the needles would be through 3D printing or laser cutting a design where the needles are bigger (not necessarily on the micro-scale) just to get our point across. After all, we just need to demonstrate that our application device will shoot the needles into something (such as cooked chicken, styrofoam, or playdoh - something that would mimic the skin). This task will be hashed out in group meetings between this and next week, before our presentation on Friday, May 9th. Our allergy test device design has come a long way from the beginning of the semester and we can't wait to show everyone how it will physically work (even if it is scaled up to get the proof of concept across).
Sunday, April 20, 2014
The future
With our design review due so soon and the graduation approaching, I can't help reflect on the information Jason presented on this week.
He gave us important information on how and where to look for jobs and how to network in the biotech area around us. As a senior graduating in May the word "future" and "job" seem scarier everyday. It felt nice to have help from someone going through the same thing. While the worry of finding a job is constant right now, knowing that not having a job by the summer isn't bad, makes me feel better.
In design review news:
I am in charge of describing the Pugh chart and how we chose our ideas.
He gave us important information on how and where to look for jobs and how to network in the biotech area around us. As a senior graduating in May the word "future" and "job" seem scarier everyday. It felt nice to have help from someone going through the same thing. While the worry of finding a job is constant right now, knowing that not having a job by the summer isn't bad, makes me feel better.
In design review news:
I am in charge of describing the Pugh chart and how we chose our ideas.
Thursday, April 17, 2014
Projector out of card box?
Yeah, no joke. I just learned that you can make a projector out of card box and a lens.
In this prototyping session, we were given some lenses, tapes, clips , crayons and a card box to make a projector. While the first idea that came to my mind was, "What?", Google told me that it's possible.
We covered all the gaps on the edges of the box, and proceeded to cut a hole that was about the shape of a given lens. The lens was then fitted into the hole. Once the phone was placed inside the box and the phone was set to have the most brightless, Voila! we couldn't see a thing.
The trick was to turn off the light. Once we did that, blurry image started to show up. Then, we adjusted the position of the phone, and also added a funnel using tape so that the air can be scattered through the lens. Overall, the projector came out pretty successful (I think).
In this prototyping session, we were given some lenses, tapes, clips , crayons and a card box to make a projector. While the first idea that came to my mind was, "What?", Google told me that it's possible.
We covered all the gaps on the edges of the box, and proceeded to cut a hole that was about the shape of a given lens. The lens was then fitted into the hole. Once the phone was placed inside the box and the phone was set to have the most brightless, Voila! we couldn't see a thing.
The trick was to turn off the light. Once we did that, blurry image started to show up. Then, we adjusted the position of the phone, and also added a funnel using tape so that the air can be scattered through the lens. Overall, the projector came out pretty successful (I think).
Feedback from Design Review 3
With the approaching deadlines of senior design projects and interviews, I have had a very busy work schedule the past two weeks. Therefore, I will combine last week's blog post with this week's post below:
Last Week (week of April 7th):
After our presentation for design review 3, we were able to get good feedback on our prototype design. Most of the comments stated how our device seemed to be close to the final product, with great works like mechanisms. One recurring comment involved how the coating of the microneedles would work and how we can possibly color code the matrix, so the allergen locations can be seen. After all, what is the point of the test if the doctor doesn't know which allergen caused any reaction? These two issues will be address in design review four and in our final report and presentation.
This week:
On Friday, we are meeting as a group to discuss the final stages of our project and how to address the remaining issues from design review 3. We will finalize our design and make sure every aspect of our design has solved all of the problems we set out to improve upon at the beginning of the semester. We will also make sure we are concise with all the aspects of the presentation, since so much has to be fit in to a 10 minute presentation.
Last Week (week of April 7th):
After our presentation for design review 3, we were able to get good feedback on our prototype design. Most of the comments stated how our device seemed to be close to the final product, with great works like mechanisms. One recurring comment involved how the coating of the microneedles would work and how we can possibly color code the matrix, so the allergen locations can be seen. After all, what is the point of the test if the doctor doesn't know which allergen caused any reaction? These two issues will be address in design review four and in our final report and presentation.
This week:
On Friday, we are meeting as a group to discuss the final stages of our project and how to address the remaining issues from design review 3. We will finalize our design and make sure every aspect of our design has solved all of the problems we set out to improve upon at the beginning of the semester. We will also make sure we are concise with all the aspects of the presentation, since so much has to be fit in to a 10 minute presentation.
Sunday, April 6, 2014
Close to Final Prototype Pictures
We have introduced two new improvements to our prototype for Design Review 3:
1) In the previous design reviews, our allergy stamp adopts a pressing mechanism. The doctor would place the allergy stamp onto the skin surface and then press down to apply the allergens. One of our classmate, Ian, had expressed a concern that the skin surface might bend in when the micro needles went down too slowly. We decided to adopt the pull and shoot mechanism, where the doctor would pull the micro needles and release to shoot them into the skin. The damping ratio as well as the spring constant must calibrated so that the spring would not bounce up and down on the skin.
2) Since the unused position of the inner plunger is in the downward position, so we also introduced a bottom cover so that the stamp can stay clean when not used.
Pictures for prototype:



1) In the previous design reviews, our allergy stamp adopts a pressing mechanism. The doctor would place the allergy stamp onto the skin surface and then press down to apply the allergens. One of our classmate, Ian, had expressed a concern that the skin surface might bend in when the micro needles went down too slowly. We decided to adopt the pull and shoot mechanism, where the doctor would pull the micro needles and release to shoot them into the skin. The damping ratio as well as the spring constant must calibrated so that the spring would not bounce up and down on the skin.
2) Since the unused position of the inner plunger is in the downward position, so we also introduced a bottom cover so that the stamp can stay clean when not used.
Pictures for prototype:
Friday, April 4, 2014
How to Read Our Allergy Test
A common question we have gotten over the past three design reviews was some variation of "How do you read the test results?". Normally, allergy tests produce small bumps on the arm called wheals and each allergen has a control bump (if there is a reaction or not) that is about 2-3mm in diameter. A positive reaction would then have a wheal size of up to 5 mm in diameter on average. The wheals can easily be seen by the eye and these sizes are measured using calipers. In our device, however, the needles are much smaller and we are scaling down the dosage of the allergens. Through research, we have found out that this change would only scale down the size of the reaction. For example, instead of a 2-3 mm control size, it might be 0.2-0.3mm (if scaled down by a factor of 10, for example). Then the reaction size might only be about 0.5 mm, which is very small. We proposed using the same caliper measuring method, but adding in a magnifying glass, so the wheals can be seen better. Many people were also skeptical about this method if we were to have a large amount of allergens in our matrix (between 10 and 40, for example).
However, after discussing with Professor Wong about this issue, she explained that the main purpose of our device is to reduce the pain of having an allergy test. Although it is important to have to read the results, we should focus on the device and how the microneedles reduce pain, not necessarily on the reading of the results. If our only design goal was to reduce the pain of having an allergy test, then all we would have to do is show that we could get the microneedles to administer a test with less pain. Therefore, we could include only 2 allergens (2 microneedle clusters on the array) just to make our point. She also mentioned how the reading of the test could also be considered a project of its own and we should just prove the pain-free administration of the test.
Therefore, I think that it is best if we just focus on making the physical/mechanical aspects of the device work and then state that by magnifying the test area, the results can be read. I also think we should address the matrix size/allergen location confusion by creating a "legend" with the microneedle arrays. I think we should have something similar to what is on a box of chocolates to say which type of chocolate is where: just a map that can be used to match the allergens to their location. In order to do this, I think we need to make the matrix not a square so the legend can still be helpful for any orientation of the array.
These are just some of the ideas I had for this one comment we seem to keep getting after design reviews and we can consider them for the final product and presentation.
However, after discussing with Professor Wong about this issue, she explained that the main purpose of our device is to reduce the pain of having an allergy test. Although it is important to have to read the results, we should focus on the device and how the microneedles reduce pain, not necessarily on the reading of the results. If our only design goal was to reduce the pain of having an allergy test, then all we would have to do is show that we could get the microneedles to administer a test with less pain. Therefore, we could include only 2 allergens (2 microneedle clusters on the array) just to make our point. She also mentioned how the reading of the test could also be considered a project of its own and we should just prove the pain-free administration of the test.
Therefore, I think that it is best if we just focus on making the physical/mechanical aspects of the device work and then state that by magnifying the test area, the results can be read. I also think we should address the matrix size/allergen location confusion by creating a "legend" with the microneedle arrays. I think we should have something similar to what is on a box of chocolates to say which type of chocolate is where: just a map that can be used to match the allergens to their location. In order to do this, I think we need to make the matrix not a square so the legend can still be helpful for any orientation of the array.
These are just some of the ideas I had for this one comment we seem to keep getting after design reviews and we can consider them for the final product and presentation.
Questions and Feedback from the Presentation
We got good responses about our device after the presentation.
One of the questions is how do we ensure that all the needles are coated with the allergens. Earlier in our brainstorming sessions we were considering adding a colored dye to the allergens solvent to see the allergens on the needles. However, if the patient is allergic to dyes, all the tests would be positives and there would not be a conclusive result. We could use a fluorescent dyes when we are testing and manufacturing the needles to show that the needles are coated and determine the percentage of the needles that end up being coated.
Another concern of the project is how to determine if the patient is allergic to the allergen or not and how to view the result. The device we are designing is mostly focused on the fast administering of the allergen and not really how to read the results. For now we are considering having the doctor observe the reaction through a magnifying glass and deciding if the patient is allergic or not. However, we don't know if reducing the dosage will make the diagnosing the allergy a yes or no reaction (if there is a reaction there is an allergy vs there is no reaction therefore there isn't an allergy).
For the moment, we are waiting for the results from the survey.
One of the questions is how do we ensure that all the needles are coated with the allergens. Earlier in our brainstorming sessions we were considering adding a colored dye to the allergens solvent to see the allergens on the needles. However, if the patient is allergic to dyes, all the tests would be positives and there would not be a conclusive result. We could use a fluorescent dyes when we are testing and manufacturing the needles to show that the needles are coated and determine the percentage of the needles that end up being coated.
Another concern of the project is how to determine if the patient is allergic to the allergen or not and how to view the result. The device we are designing is mostly focused on the fast administering of the allergen and not really how to read the results. For now we are considering having the doctor observe the reaction through a magnifying glass and deciding if the patient is allergic or not. However, we don't know if reducing the dosage will make the diagnosing the allergy a yes or no reaction (if there is a reaction there is an allergy vs there is no reaction therefore there isn't an allergy).
For the moment, we are waiting for the results from the survey.
Friday, March 28, 2014
Needles and Antigen Delivery
As John mentioned yesterday there are a few needle ideas we have in mind.
The first is coating a solid needle with an antigen layer which will dissolve and stay in the body. We have concerns about how exactly the layer would dissolve and how long it would take. This method is currently being researched in MIT to deliver DNA vaccines with microneedles.
Another idea is to have a hollow needle with the antigen in the needle. A water soluble polymer would block the hole to prevent leakage. Once the needle is inserted into the skin, the polymer would dissolve and the antigen liquid would leak out. We would have to choose a polymer that dissolves almost instantly when it reaches extracellular matrix in the body to have fast delivery of the antigen.
Another idea is having 2 layers in the microneedle pad. A top layer that contains the microneedles and a lower layer that contains pouches with the antigens. When the top of the device is clicked, the microneedles will lower to reach and pop the pouches and then pierce the skin. How do we know the liquid in the pouch actually reaches the inside of the body?
Another is a combination of the last two ideas. Having the pouches inside a primary hollow needle that has another needle inside the primary needle. When device is pushed and reached the body, the internal needle will pop the internal pouch and the hollow needle will direct where the antigen liquid goes. The concern would be how to manufacture the needles.
We are currently discussing the designs of the needles and how the manufacturing of each will maintain the cost reasonable.
The first is coating a solid needle with an antigen layer which will dissolve and stay in the body. We have concerns about how exactly the layer would dissolve and how long it would take. This method is currently being researched in MIT to deliver DNA vaccines with microneedles.
Another idea is to have a hollow needle with the antigen in the needle. A water soluble polymer would block the hole to prevent leakage. Once the needle is inserted into the skin, the polymer would dissolve and the antigen liquid would leak out. We would have to choose a polymer that dissolves almost instantly when it reaches extracellular matrix in the body to have fast delivery of the antigen.
Another idea is having 2 layers in the microneedle pad. A top layer that contains the microneedles and a lower layer that contains pouches with the antigens. When the top of the device is clicked, the microneedles will lower to reach and pop the pouches and then pierce the skin. How do we know the liquid in the pouch actually reaches the inside of the body?
Another is a combination of the last two ideas. Having the pouches inside a primary hollow needle that has another needle inside the primary needle. When device is pushed and reached the body, the internal needle will pop the internal pouch and the hollow needle will direct where the antigen liquid goes. The concern would be how to manufacture the needles.
We are currently discussing the designs of the needles and how the manufacturing of each will maintain the cost reasonable.
Thursday, March 27, 2014
Design Review 3 Tasks
After class today, we had some good conversations with each other and with another classmate about how to approach our final design. Although we do need to improve on our design for the final report, our first prototype seemed to be pretty "works-like" with the spring mechanism for the stamp. The new additions for design review 3 that we need to work on include the FMEA for the device and the regulatory strategy. Since we began the FMEA analysis during class on Tuesday, that just needs to be completed and shouldn't take too long. As for the regulatory strategy, the FDA website (fda.gov) should have plenty of information on how to classify our device. Two devices I found that we could possibly use to help us classify our device include the Fluzone Intradermal, which is a flu vaccine delivered by a microneedle, and the DermaRoller, which is a roller containing many microneedles that get rolled onto the skin. We have also mentioned in previous posts the patents that are out there now for different kinds of research with microneedles as a drug delivery system. I think this is plenty of information to start us out with a regulatory strategy for our allergy testing product.
Pointers on Tips
At the end of class today, we got a chance to pull Ian aside. Ian had brought up some points about our microneedle device after design review 2, and we got him to give us some pointers on how to fabricate the allergen tips. For the most part, we've been considering our microneedles in terms of where they're going, into the dermis of the skin, and how the allergen is going to be delivered once they're there, either by hollow tubes, coated solid microneedles, or encapsulated tips. However, Ian raised a lot of red flag about what it actually takes to fabricate these microneedles. He is currently working on a senior project that works with microneedles and might even involve developing an applicator.
One problem he brought up was the flexing of the skin by a sort of bed-of-nails effect where the array sits on the skin, bending it slowly rather than puncturing quickly. We've talked about this before, and Ian wasn't even sure it would be a problem for our application. We should hash that out with real examples because his example of the Surgilance doesn't really fit our goals. Surgilance and Ian are both more interested in blood withdrawal rather than drug delivery.
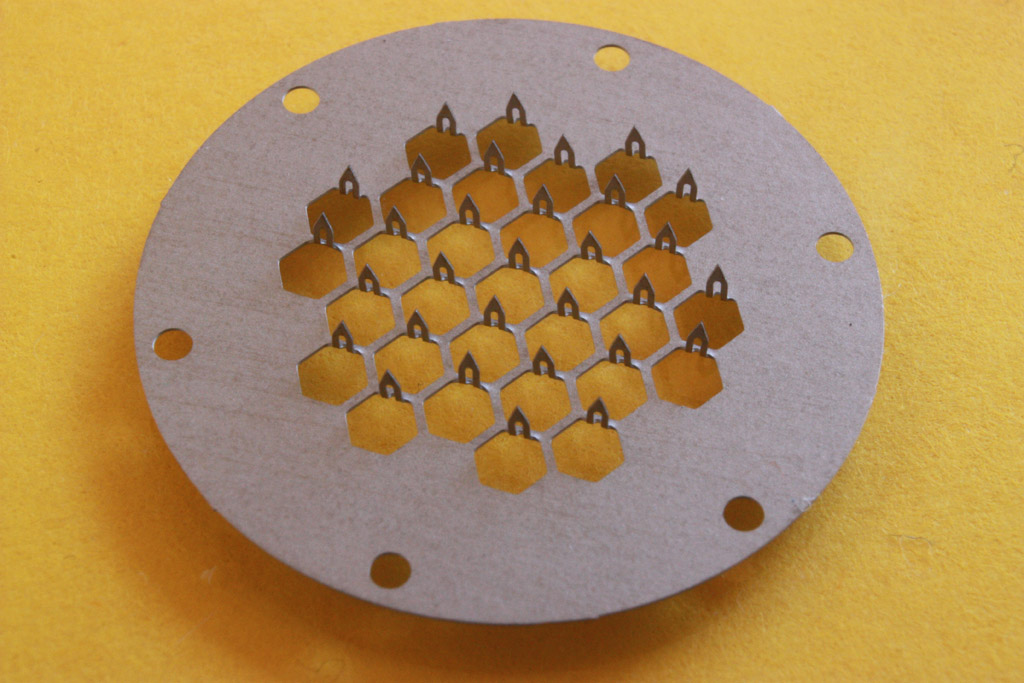
Another problem he brought up is fabrication. Based on available industrial methods, some of the more complex tips might be a pipe dream. He suggested a printed sheet where needles are bent up. This image gets the idea across. It's not the ideal picture were were thinking of, but it might end up being the more reasonable route. It asks important questions about our product. Are we making something that anticipates future manufacturing methods, or do we want something that'll be ready to go our the door with available methods? The latter makes a lot more sense for this class and the lessons we've learned from it. We're not just making a feasible laboratory device; we need a marketable product that at least theoretically attract investors.
One problem he brought up was the flexing of the skin by a sort of bed-of-nails effect where the array sits on the skin, bending it slowly rather than puncturing quickly. We've talked about this before, and Ian wasn't even sure it would be a problem for our application. We should hash that out with real examples because his example of the Surgilance doesn't really fit our goals. Surgilance and Ian are both more interested in blood withdrawal rather than drug delivery.
Another problem he brought up is fabrication. Based on available industrial methods, some of the more complex tips might be a pipe dream. He suggested a printed sheet where needles are bent up. This image gets the idea across. It's not the ideal picture were were thinking of, but it might end up being the more reasonable route. It asks important questions about our product. Are we making something that anticipates future manufacturing methods, or do we want something that'll be ready to go our the door with available methods? The latter makes a lot more sense for this class and the lessons we've learned from it. We're not just making a feasible laboratory device; we need a marketable product that at least theoretically attract investors.
{kind=link}
Wednesday, March 26, 2014
In-class activity: Tracheotomy
Yesterday, we had our second prototyping session. Unlike last time, we were not given any material to start with. Instead, we were told to improvise a tracheotomy kit out of the items that we could find on us.
Here's the list of items that we found:
John: 2 pen caps
Natalia: A knife looking bookmark
David: A plastic straw from his bottle
Lauren: Hand sanitizer
Brian: Sharp ended floss and CD
Me: Manual and bag for the kit
(Sorry if i missed something)
With all these items, we came up with the following Tracheotomy kit:
Manual:
1) Apply hand sanitizer to sanitizer area
2) Break CD into half for sharp edges
3) Using broken CD, floss's sharp tip, and knife looking bookmark to cut open the skin and tissues until the trachea is reached
4) With the clip on the pen caps, clip open the cut on the neck to stabilize/ ply open the opening
5) When the trachea is reached, push in the straw to allow breathing of the patient
6) Apply hand sanitizer to disinfect area.
I personally think the kit turned out to be pretty well, and it was well explained by the other group members.
Here's the list of items that we found:
John: 2 pen caps
Natalia: A knife looking bookmark
David: A plastic straw from his bottle
Lauren: Hand sanitizer
Brian: Sharp ended floss and CD
Me: Manual and bag for the kit
(Sorry if i missed something)
With all these items, we came up with the following Tracheotomy kit:
Manual:
1) Apply hand sanitizer to sanitizer area
2) Break CD into half for sharp edges
3) Using broken CD, floss's sharp tip, and knife looking bookmark to cut open the skin and tissues until the trachea is reached
4) With the clip on the pen caps, clip open the cut on the neck to stabilize/ ply open the opening
5) When the trachea is reached, push in the straw to allow breathing of the patient
6) Apply hand sanitizer to disinfect area.
I personally think the kit turned out to be pretty well, and it was well explained by the other group members.
Saturday, March 22, 2014
A New Prototype?
Our current prototype utilizes a plunger that allows the user to apply the needle pad at an evenly distributed pressure of their choice. It may be the case that an alternate application method may be more appropriate. For instance, we received feedback from a classmate who has experience with microneedles that the needles should be injected quickly. If they are injected too slowly, the skin surface can bend, which he surmised would be a bad thing. One potential problem with the skin bending is that there may be a less even distribution of needles across the skin. Or perhaps the allergen would not be injected at the correct depth. Thus, we have considered spring-loaded designs that can "shoot" the needles into the skin. Such a mechanism could be initiated by a click at the top of the applicator or even at the bottom of the applicator as it comes into the surface of the skin. I have some rough sketches that I will post as soon as I can scan them. After further discussion and consideration, we may look to translate the sketches into CAD drawings and look to 3-d print.
Thursday, March 20, 2014
Weekly Update: Return from Spring Break
Over spring break, I had the chance to speak with another friend who really emphasized how much a less painful allergy test would benefit anyone who has to go through the testing. I know we were aiming toward a product to help children with allergy testing, but I think this we have a good chance of marketing this to all people who get allergy tests. She also explained how when she got tested, they first tested her for general categories of allergies to see what group of allergens she was allergic to. After that, they tested her for the specific allergens in that group. Maybe we could design different allergy pads with like 10 or 20 allergens that are in groups. That way, if the person is suspected to have a certain allergy, there can be specific pads for that allergen group. We could also still do an allergy pad with unrelated allergens, then go into the more specific allergen tests. This was just my thought for the week after talking to a patient who recently had the testing done. Obviously once the prototype design is complete and we can figure out the size of the matrix, we will know how many allergens each pad can contain. Only then can we look into this specification for our product.
I have also created a logo for our product. It's a work-in-progress, but does a pretty nice job making the bee look friendly, as opposed to hurtful :)

I have also created a logo for our product. It's a work-in-progress, but does a pretty nice job making the bee look friendly, as opposed to hurtful :)
Changing of our major focus of the project
We talked to Prof. Wong, and she suggested that we should focus on the reducing pain / standardizing the produce, rather than focusing too much on the diagnosis part of the project.
So, we decided to lower the number of allergens being tested by the device. Also, our primary contact told us that for most of the time, doctors already have an idea what type of allergens might be causing the allergic reaction, so they can just choose the specific allergens needed to perform the allergy testing.
Friday, March 7, 2014
Very Useful Paper for Microneedle Choices
This hyperlinked journal article is a review of microneedles for drug and vaccine delivery. I believe we've passed this around before, but I don't think we've featured it on the blog. There are certainly still lessons we can learn from it.
We can channel this primary information into our particular application. It talks about each choice of microneedle geometry, material, and drug delivery type. Some drug delivery devices are better suited for other applications. For example,fully dissolvable poly-saccharide subtrate microneedles are very effective for drug delivery in flu vaccine applications and limits biohazardous waste. However, that application requires a 10 minute set time in which the patch is constantly in contact with the arm. While this is fine for drug delivery, that 10 minutes of patch contact may disrupt the measurable outcome of the scratch test and render the assay useless. Those are the sorts of choices that we can propose and mark of the list. We have spoken in general and sometimes more specific terms about these choices and think we have an idea of what suits our project, but we should give this article rigorous consideration so that we may make the most appropriate choice. Perhaps there are recently developed geometries and subtrates that competitors neglected or weren't priviledge to. We have the advantage that the competitors that have approached this problem had to make final design choices earlier, where current research and manufacturing capacity could now be better suited.
Take a look at the paper! Future posts will have a more comprehensive analysis.
In case you missed the hyperlink: http://drugdelivery.chbe.gatech.edu/Papers/2012/Kim%20Adv%20Drug%20Deliv%20Rev%202012.pdf
We can channel this primary information into our particular application. It talks about each choice of microneedle geometry, material, and drug delivery type. Some drug delivery devices are better suited for other applications. For example,fully dissolvable poly-saccharide subtrate microneedles are very effective for drug delivery in flu vaccine applications and limits biohazardous waste. However, that application requires a 10 minute set time in which the patch is constantly in contact with the arm. While this is fine for drug delivery, that 10 minutes of patch contact may disrupt the measurable outcome of the scratch test and render the assay useless. Those are the sorts of choices that we can propose and mark of the list. We have spoken in general and sometimes more specific terms about these choices and think we have an idea of what suits our project, but we should give this article rigorous consideration so that we may make the most appropriate choice. Perhaps there are recently developed geometries and subtrates that competitors neglected or weren't priviledge to. We have the advantage that the competitors that have approached this problem had to make final design choices earlier, where current research and manufacturing capacity could now be better suited.
Take a look at the paper! Future posts will have a more comprehensive analysis.
In case you missed the hyperlink: http://drugdelivery.chbe.gatech.edu/Papers/2012/Kim%20Adv%20Drug%20Deliv%20Rev%202012.pdf
Thursday, March 6, 2014
Design Review 2 Process and Feedback
After discussing our second design review, which included our prototype and visions for the final product, we came up with some useful feedback and potential issues. One thing we need to consider for the final design is the pressure used to apply the microneedles to the patient; we tried to address this problem by creating an applicator attachment to stabilize the device. We also designed a groove in the device so the plunger can only get pushed down to a certain distance. However, those do not standardize the amount of pressure a doctor uses to physically push the button down. We were also reminded that if we use microneedles, they have to be injected into the patient fast, in order to reduce the risk of the arm/skin bending before insertion. The next part of our design phase would have to focus on these issues and provide a solution that stays true to our original stamp design.
I have found two articles that address the issue with the force applied to microneedles for insertion into the skin. They can be found here and here. Both of these research articles discuss the force thresholds: a minimum force must be applied, but there is also a maximum force they can reach before breaking. This is something to consider if we do not use dissolvable or biodegradable microneedles. These are just some more quantitative angles we have to look at for our design and how we can get it to function properly.
I have found two articles that address the issue with the force applied to microneedles for insertion into the skin. They can be found here and here. Both of these research articles discuss the force thresholds: a minimum force must be applied, but there is also a maximum force they can reach before breaking. This is something to consider if we do not use dissolvable or biodegradable microneedles. These are just some more quantitative angles we have to look at for our design and how we can get it to function properly.
Sequence Drawings
How to set up our device:
.jpg) |
The stabilizer is screwed off to expose the pad holder and the pad is then attached.
|
.jpg) |
| The stabilizer is then reattached to the rest of the applicator and can be used. |
How to use our device:
 |
| The area where the allergy test will be done is cleaned. |
 |
| The applicator is placed on the area and the button on the top is pushed to inject the needles. |
 |
| The button is then released and the needles will rise off the skin. |
 |
| The applicator is removed from the skin and a matrix is left on skin to indicate where the needles were inserted. |
 |
| The stabilizer is once again removed |
 |
| The used pad is then removed into a biohazard container. |
Tuesday, March 4, 2014
CAD drawing
In the past few weeks, I've been learning SolidWorks and trying to come up with a model for the stamp. This is what I've come up with so far.


Friday, February 28, 2014
Future questions
We have come up with the general idea of how our product should look like as seem in previous posts. We however did to figure out how it would work.
One idea is to coat the needles with the necessary allergen by having the needles be the opposite charge as the allergen. This will help the coating stay in the body when the needles are removed.
Are we able to have the same concentration and dose on the needles that are being used with current allergy tests?
Will having microneedles remove the reaction of the control meaning the only reaction will be the body reaction to the present allergen?
If not, how will be judge if there is an allergic reaction or not?
These are questions that need to be researched and answered moving forward.
One idea is to coat the needles with the necessary allergen by having the needles be the opposite charge as the allergen. This will help the coating stay in the body when the needles are removed.
Are we able to have the same concentration and dose on the needles that are being used with current allergy tests?
Will having microneedles remove the reaction of the control meaning the only reaction will be the body reaction to the present allergen?
If not, how will be judge if there is an allergic reaction or not?
These are questions that need to be researched and answered moving forward.
Thursday, February 27, 2014
Next Steps for the Project
So far this semester, we have come up with some great ideas for designing our allergy stamp test. We have an idea of what the device as a whole should look like and how it should function, as seen in previous blog posts. Our next steps will be to figure out the technical aspects of the device, such as the concentration of allergen we need to observe a meaningful result (reaction or no reaction). We also need to decide how much allergen each microneedle could contain, so we can figure out how many needles would be necessary to have the proper concentration for each allergen. The last major technical aspect we need to figure out is how the reactions will be detected; whether we will get bumps that can be seen through a lens (like a magnifying glass), or whether an automated system needs to be used. All of these things will be addressed over the next week, with the hopes of hashing out the final technical details of our device.
Tuesday, February 25, 2014
Another Reference
Last week I found another reference for our project. I talked to Pediatrician Dr. Elias Milgram this is his website: < http://www.drmilgram.com/Home > Dr. Milgram offered himself to help us in our further development of the product by giving feedback on the medical point of view of our product development. He is an extremely talented and a well known doctor among the Pediatric community. Dr. Milgram currently works in Miami, FL. In my last interview with him, Dr. Milgram claimed to be interested on our product and believed on the feasibility of our idea. Nonetheless, he stressed on the importance of having the right pressure for the needles to reach the skin deepness required. Moreover, he also pointed the relevance of having a way of standardizing the test in some way so that allergologists can actually make diagnostics based on the wheal size.
Monday, February 24, 2014
Pitfalls of Skin Prick Testing in Food Allergy Diagnosis
Here's a paper on skin prick testing (SPT) and its pitfalls: http://www.ncbi.nlm.nih.gov/pubmed/20922509
(be sure you're on BU network or VPN)
It explores the process of food allergy diagnoses and therapies in detail and concludes that the placebo-controlled oral food challenge is the gold standard in food allergy diagnosis. We should consider the merits of their arguments against our product and determine which food allergens are compatible with the skin prick test. Because our product works within the same theoretical framework as the skin prick test, we can evaluate our method with the same lens. However, we must also consider the improvements we make, such as the claim of increases specificity due to careful control of the application. Perhaps we can address their claims that current uses of SPT and serum food-specific IgE are insufficient without careful medical histories. Maybe we can knock some gold standards out of place!
(be sure you're on BU network or VPN)
It explores the process of food allergy diagnoses and therapies in detail and concludes that the placebo-controlled oral food challenge is the gold standard in food allergy diagnosis. We should consider the merits of their arguments against our product and determine which food allergens are compatible with the skin prick test. Because our product works within the same theoretical framework as the skin prick test, we can evaluate our method with the same lens. However, we must also consider the improvements we make, such as the claim of increases specificity due to careful control of the application. Perhaps we can address their claims that current uses of SPT and serum food-specific IgE are insufficient without careful medical histories. Maybe we can knock some gold standards out of place!
Sunday, February 23, 2014
First time trying out CAD
I've spent my entire day trying to figure out something with CAD, and this is my first very very very rough sketch.


Saturday, February 22, 2014
Device Design
Last week, I took some time to consider how some basic characteristics of the device's design would be carried out. In addition to looking to create a microneedle patch, our team aims to develop a way to apply the patch. By shifting contexts and investigating things like stamps and clickable pens, we can get some inspiration. I've sketched some possible designs based that are based off a similar mechanism that clickable pens use. While developing possible ideas, it is important to keep the design as simple and as easy to implement as possible. I'll post some sketches soon when I have the means to scan them.
Thursday, February 20, 2014
Preliminary Designs
After attempting to do a sequence drawing schematic of how our device would be used during class, we all decided that we need to have a clear understanding of how our device functions. We also need to figure out whether or not we will use biodegradable microneedles, whether we will inject the allergen through these microneedles, or whether we will just coat the microneedles with the allergen. We also have to figure out the most common allergies we should test for using this stamp.
According to this Mother Nature Network article, the 9 most common allergies are the following:

According to this Mother Nature Network article, the 9 most common allergies are the following:
1. Wheat
2. Penicillin
3. Eggs
4. Pet Dander (for cats and dogs)
5. Mold
6. Milk
7. Pollen
8. Peanuts
9. Sun
Obviously, we won't be able to test for some of these allergies, such as milk, by using a test like ours, but this list is a start. As an example, our device could have a matrix containing 8 allergens and 1 control. Below are some preliminary designs I have created on the basic shape of the stamper and allergen matrix.
Wednesday, February 19, 2014
The Nitty Gritty
After getting through intensive ideation and finally making an idea, we have been dealing with the specific details of our product. We decided to keep a running list of issues and topics that need to be dealt with in more detail, and we have been volunteering to take on individual research goals. The idea is that each person will naturally be familiar with the project as a whole, but each task calls for more care than six people could efficiently offer. So, while we are taking new developments as they arrive--and they arrive quickly--we are simultaneously trying to bring structure to our work.
David gathered our ideas in a list on our Facebook page, and we each elected to focus on one of following:
1. Determine the size of our prototype and concentration of
allergen required.
2. Do a rough sketch of the product by hand and possibly in
CAD
3. Determine how the needles will be distributed and spaced
4. Do a logo and pick colors for the product
5. Determine how to insert the allergen in the needles/patch
6. Determine the material of the stamp, patch, and which
microneedles to use. Also how to adhere the stamp to the patch.
7. Determine which lens to use or what technology to use to
capture the size of the skin reaction.
The list is incomplete, representing a snapshot of what
seemed urgent at the time, which has changed and continues to change. I
think that the list has a lot of potential as a living document that grows
alongside our project. The more we learn, the our answers to problems, as well
as problems themselves, develop and take on new form. By the end of the
project, we will have an extensive list of problems and researched solutions,
and presenting the work to others will hopefully be trivial.
Saturday, February 15, 2014
Weekly Update
So... time to post again for the weekly update. While Natlia's previous blog entry addressed some of the questions from Design Review presentation, I will focus on some of the comments/suggestions given in the feedback.
This summarizes some of the comments/suggestions
Convincing Need?
1) More stats.
- How many people have un-diagnosed allergies?
2) Pain reduction doesn't seem to be that pressing of a need.
Reasonable Specs?
1) In addition to cutting down on test duration, aim to cut down on diagnostic time as well.
2) Specificity/Sensitivity?
3) Don't necessarily limit testing to children, as some allergies don't develop until later
Creative Ideas?
1) Use microneedles to draw blood - then use lateral flow test
2) Microfluid device to collect and analyze blood samples
Likable Features?
1) Reduced pain
2) Quickly tests multiple allergens
Potential Challenges?
1) maintaining structural integrity
2) producing prototype of accurate proportions (on micrometer scale)
3) interpreting results - ie diagnosing correct allergens (avoid contamination)
4) determining amount of allergen necessary to deliver
Other Comments/Questions? -
1) Could this ever be safe for at home testing? What if allergic reaction occurs?
2) Make table of each allergen being tested and method of testing
3) Use input from contacts to find out feasible needle density
Suggested Contacts?
1) Kristine Krol - Allergy Specialist
2) People with allergies - feedback on comfort, hesitations, etc
3) Check Boston Children's and Harvard Vanguard
4) Johnathan Rosen - BME technology commercialization
We'll look into these and try to better address our solutions!
This summarizes some of the comments/suggestions
Convincing Need?
1) More stats.
- How many people have un-diagnosed allergies?
2) Pain reduction doesn't seem to be that pressing of a need.
Reasonable Specs?
1) In addition to cutting down on test duration, aim to cut down on diagnostic time as well.
2) Specificity/Sensitivity?
3) Don't necessarily limit testing to children, as some allergies don't develop until later
Creative Ideas?
1) Use microneedles to draw blood - then use lateral flow test
2) Microfluid device to collect and analyze blood samples
Likable Features?
1) Reduced pain
2) Quickly tests multiple allergens
Potential Challenges?
1) maintaining structural integrity
2) producing prototype of accurate proportions (on micrometer scale)
3) interpreting results - ie diagnosing correct allergens (avoid contamination)
4) determining amount of allergen necessary to deliver
Other Comments/Questions? -
1) Could this ever be safe for at home testing? What if allergic reaction occurs?
2) Make table of each allergen being tested and method of testing
3) Use input from contacts to find out feasible needle density
Suggested Contacts?
1) Kristine Krol - Allergy Specialist
2) People with allergies - feedback on comfort, hesitations, etc
3) Check Boston Children's and Harvard Vanguard
4) Johnathan Rosen - BME technology commercialization
We'll look into these and try to better address our solutions!
Friday, February 14, 2014
Resource for learning CAD
In response to Lauren, I agree that our current primary contacts are very solid. One of them is an allergist, who has intensive experience with allergy testing. I believe that David did a good job listing out the aspects that we should prioritize on.
I would like to recommend lynda.com to any of you who wants to learn solidworks, their tutorials are super informative and helpful, and you can essentially learn every software/ programming language from it. It costs $25, BUT you can use it for free if you have a friend/family member who goes to a college that has free access to lynda and is willing share with you. These colleges include northeastern, Emory, columbia, carnegie mellon, american university, and tons of others. Just search for the schools' name followed by lynda.com to see if that college has access to the site. Annoyingly, BU doesn't have it.
I would like to recommend lynda.com to any of you who wants to learn solidworks, their tutorials are super informative and helpful, and you can essentially learn every software/ programming language from it. It costs $25, BUT you can use it for free if you have a friend/family member who goes to a college that has free access to lynda and is willing share with you. These colleges include northeastern, Emory, columbia, carnegie mellon, american university, and tons of others. Just search for the schools' name followed by lynda.com to see if that college has access to the site. Annoyingly, BU doesn't have it.
Things to do:
After receiving feedback from the class, professor, and doctors. We are looking forward to improve our product. For now, these are some of the things we have to do next:
1. Determine the size of our prototype and concentration of allergen required.
2. Do a rough sketch of the product by hand and possibly in CAD
3. Determine how the needles will be distributed and spaced
4. Do a logo and pick colors for the product
5. Determine how to insert the allergen in the needles/patch
6. Determine the material of the stamp, patch, and which micro needles to use. Also how to adhere the stamp to the patch.
7. Determine which lens to use or what technology to use to capture the size of the skin reaction.
1. Determine the size of our prototype and concentration of allergen required.
2. Do a rough sketch of the product by hand and possibly in CAD
3. Determine how the needles will be distributed and spaced
4. Do a logo and pick colors for the product
5. Determine how to insert the allergen in the needles/patch
6. Determine the material of the stamp, patch, and which micro needles to use. Also how to adhere the stamp to the patch.
7. Determine which lens to use or what technology to use to capture the size of the skin reaction.
Thursday, February 13, 2014
Microneedle Technology Article
Just last year, the Discovery channel had an article about a microneedle patch for delivering vaccines. It is just an example about how our idea is plausible and is in line with current emerging technologies. Click here for the Discovery News article.
In other news, I finally got a response back from my dad's cousin, who is a doctor at Beth Israel Deaconess Medical Center, but she said she does not have much experience with allergy testing. She also does not have experience getting her children tested for allergies, so she couldn't attest to the pain children experience. It was worth a try, but I think our other contacts are pretty solid.
- Lauren
In other news, I finally got a response back from my dad's cousin, who is a doctor at Beth Israel Deaconess Medical Center, but she said she does not have much experience with allergy testing. She also does not have experience getting her children tested for allergies, so she couldn't attest to the pain children experience. It was worth a try, but I think our other contacts are pretty solid.
- Lauren
Tuesday, February 11, 2014
After Progress Presentation
These are the main aspects people asked about after the presentation:
How do we put multiple needles without affecting the reactions?
We're going to need to see if there is a ratio to how close the needles can be to each other in terms of concentration of the allergen.
What if a microneedle breaks in the body?
We can consider making the microneedles biodegradable for disposal and if the needles get stuck in the body.
Is it painful?
While the aspect of having multiple needles in the body seems painful, products having microneedles have said they aren't painful.
How will the reaction be detected?
There are detection devices with other microneedle allergy tests which scan the area and determine if there is a reaction. The doctor could maybe measure the reaction by using a magnifying glass. Maybe since the needles are smaller, the only bumps that form will be from allergy reactions. Maybe we could use a lotion or something depending on the heat of the reaction or antibodies from the small wound. We need to consider and discuss further how the detection will be determined.
Other than these concerns, the product seemed to be well received. We will now need to wait for the evaluations from our peers.
How do we put multiple needles without affecting the reactions?
We're going to need to see if there is a ratio to how close the needles can be to each other in terms of concentration of the allergen.
What if a microneedle breaks in the body?
We can consider making the microneedles biodegradable for disposal and if the needles get stuck in the body.
Is it painful?
While the aspect of having multiple needles in the body seems painful, products having microneedles have said they aren't painful.
How will the reaction be detected?
There are detection devices with other microneedle allergy tests which scan the area and determine if there is a reaction. The doctor could maybe measure the reaction by using a magnifying glass. Maybe since the needles are smaller, the only bumps that form will be from allergy reactions. Maybe we could use a lotion or something depending on the heat of the reaction or antibodies from the small wound. We need to consider and discuss further how the detection will be determined.
Other than these concerns, the product seemed to be well received. We will now need to wait for the evaluations from our peers.
Sunday, February 9, 2014
Explaining our Idea
As Natalia previously mentioned, our idea combines a micro needle patch that administers the drugs and the stamp that avoids the idea of having the patch attached to our skin for many hours. The combination of the patch and stamp enables the patients to test for different allergens without having the painful and invasive procedures of nowadays allergy tests. The VACC-STAMP injects the drug in a very subtle way by exposing its micro needles that are attached to the patch. The patch contains a matrix of different allergens and a mixture of anti-inflammatory/disinfectants that administer the drug and prevent infection. This new product is convenient for doctors and patients because:
- It administers the drug easier and faster
- It can be used in any kind of patient
- It replaces the painful and invasive current allergy tests
- It is cleaner and prevents infection
- It extremely easy to use
- It is portable
These are some of the characteristics that describe our product and that make us believe that this patch & stamp technology can have a great impact on the health diagnostics market.
Our next step is to consult doctors and professionals about the feasibility of the product.
- It administers the drug easier and faster
- It can be used in any kind of patient
- It replaces the painful and invasive current allergy tests
- It is cleaner and prevents infection
- It extremely easy to use
- It is portable
These are some of the characteristics that describe our product and that make us believe that this patch & stamp technology can have a great impact on the health diagnostics market.
Our next step is to consult doctors and professionals about the feasibility of the product.
Friday, February 7, 2014
Finding a plausible idea!
While looking for diagnostic problems, we decided to focus on a less painful way of diagnosing allergies.
Currently, there are three ways to diagnose allergies: skin prick test, interdermal test, and skin patch test. To do a skin prick test a drop of an allergen solution is placed on the skin and then a needle prick is applied allowing for the solution to enter the skin. Similarly, an interdermal test is done by injecting an allergen solution into the skin. A skin path is when a pad with an allergen solution is placed on the skin. For all there are two ways to determine an allergy, a blood test where the concentration of antibodies is calculated and a skin reaction test where the size of the reaction is measured.
Our first idea was to create a microneedle interdermal patch that attaches to the skin and after a certain time period is removed and the results can be seen on the skin. This idea however was found to be currently patented.
Our second and current idea is to combine the patch idea with a stamp. Therefore the allergen can be injected into the skin using microneedles on a stamp. This will take less time to administer and can be used on children. A similar idea currently in testing is called a Vacc-Stamp which uses microneedle vaccines on babies.
We are currently still developing this idea more.
Currently, there are three ways to diagnose allergies: skin prick test, interdermal test, and skin patch test. To do a skin prick test a drop of an allergen solution is placed on the skin and then a needle prick is applied allowing for the solution to enter the skin. Similarly, an interdermal test is done by injecting an allergen solution into the skin. A skin path is when a pad with an allergen solution is placed on the skin. For all there are two ways to determine an allergy, a blood test where the concentration of antibodies is calculated and a skin reaction test where the size of the reaction is measured.
Our first idea was to create a microneedle interdermal patch that attaches to the skin and after a certain time period is removed and the results can be seen on the skin. This idea however was found to be currently patented.
Our second and current idea is to combine the patch idea with a stamp. Therefore the allergen can be injected into the skin using microneedles on a stamp. This will take less time to administer and can be used on children. A similar idea currently in testing is called a Vacc-Stamp which uses microneedle vaccines on babies.
We are currently still developing this idea more.
Thursday, February 6, 2014
Nebulizing Creative Hurdles
Tuesday's group breakout exercise,
rapidly prototyping an electricity-free and child-friendly nebulizer, helped me
realize a lot of deficiencies in my approach to creative problems and
underlined some important issues in operating effectively as a team. From the
start of the workshop, it was clear to me how we were going to get the
nebulizer to work: pump connects to tubes connects to inhalation device, throw
in connecting pieces, plug holes, get out the door in under two minutes. For
the most part, that is what happened, but it was just as straightforward for
everyone else. I was too focused on the idea of jumping in and getting the
thing to work period that I missed out on some really simple ideas to make our
product approachable and fitting for its application.
The presentations showed how a few
simple creative ideas could really set the product apart from its competitors
and cater the way it is used by the user. Something as simple as making the
mouthpiece less intimidating for the child with a an animal shape, as one group
did with a dragon, or, as another group did, using the T-junction and a second
pump to create a continuous stream could greatly enhance the user experience
and even make it more attractive than the electrically-pumped device.
Moreover, I realized that those
simple ideas would be a lot easier to come across if we made better use of each
other as a team. We could definitely use some practice in decreasing friction and
letting ideas flow more freely. I feel as if we squelch ideas a little too
quickly, and we sometimes abandon ones that, in hindsight, may have been
promising leads or at least a route to later branch off from. A major part of
why I am in this course is to gain those skills, especially in the context of engineering,
and to get into the groove of getting the most out of group projects like this.
Let us hope we do that!
Brainstorming - The Ideas that Didn't Make It
Brainstorming can be tough... Especially when attempting to implement a novel diagnostic device. Over the last week or so, I've been trying to think of innovative ideas. I've tried several strategies: combining existing technologies, thinking back to previous projects or labs I've worked on, evaluating existing diagnostic protocols, shifting contexts... Despite coming up with several ideas they all had their flaws and didn't seem to catch on with the rest of the group. Here's a couple examples.
Building off of previous lab experience, I considered a sleep monitoring device. After all, there are many easy to measure and informative biological signals during sleep. These include ECG, EMG, EEG, and EOG data. These signals vary through the night in each shift of sleep cycle. With careful monitoring of such signals, one could see if anything was irregular in their sleep pattern. For instance, too long or too short of time spent within REM can greatly affect mood, alertness, memory, and many other conditions. Our device could monitor one or more of a subject's biological signals and be programmed to analyze and interpret the data and present its results in a useful, user-friendly form.
Another idea came to me when considering a semi-neglected problem: HPV in men. HPV is very common and most sexually active people will have it at some point in their life. High risk types of HPV can cause cervical, anal, penile or throat cancer. Lower risk types which don't cause cancer can cause genital warts. Overall however, symptoms are rare, and the virus will typically go away on its own within a couple of years. Women after the age of 30 are recommended to get tested regularly: a pap test and an HPV test. The HPV test tells whether the patient has the virus. Having the virus alone is not considered overly problematic, as it typically goes away on its own without symptoms. The pap test checks for irregular cell morphology that could lead to cancer. Having a positive pap test is more reason for concern. There's no recommended test for men, due to how rare symptoms are. However, as rare as it is, due to the large number of people that get HPV, approximately 8,400 people within the US are diagnosed with oropharyngeal cancer that may be caused by HPV. Men are approximately 3 times more likely than women to get this type of cancer. Thus, despite the fact that oroparyngeal cancer is "rare," it still affects a great amount of people. In addition to men having no regular screening, there is no approved test (for men or women) to find HPV in the mouth or throat. Since over screening is an economic concern, a cheap, perhaps self/home test could have potential.
Building off of previous lab experience, I considered a sleep monitoring device. After all, there are many easy to measure and informative biological signals during sleep. These include ECG, EMG, EEG, and EOG data. These signals vary through the night in each shift of sleep cycle. With careful monitoring of such signals, one could see if anything was irregular in their sleep pattern. For instance, too long or too short of time spent within REM can greatly affect mood, alertness, memory, and many other conditions. Our device could monitor one or more of a subject's biological signals and be programmed to analyze and interpret the data and present its results in a useful, user-friendly form.
Another idea came to me when considering a semi-neglected problem: HPV in men. HPV is very common and most sexually active people will have it at some point in their life. High risk types of HPV can cause cervical, anal, penile or throat cancer. Lower risk types which don't cause cancer can cause genital warts. Overall however, symptoms are rare, and the virus will typically go away on its own within a couple of years. Women after the age of 30 are recommended to get tested regularly: a pap test and an HPV test. The HPV test tells whether the patient has the virus. Having the virus alone is not considered overly problematic, as it typically goes away on its own without symptoms. The pap test checks for irregular cell morphology that could lead to cancer. Having a positive pap test is more reason for concern. There's no recommended test for men, due to how rare symptoms are. However, as rare as it is, due to the large number of people that get HPV, approximately 8,400 people within the US are diagnosed with oropharyngeal cancer that may be caused by HPV. Men are approximately 3 times more likely than women to get this type of cancer. Thus, despite the fact that oroparyngeal cancer is "rare," it still affects a great amount of people. In addition to men having no regular screening, there is no approved test (for men or women) to find HPV in the mouth or throat. Since over screening is an economic concern, a cheap, perhaps self/home test could have potential.
Tuesday, February 4, 2014
Weekly update from Tim.
We've come up with many different ideas from brainstorming. I have experience with App development, so our original brainstorming revolved around making an app that helps diagnose something. But we later ended up choosing to tackle allergy testing, because we found it more fitting to the group as a whole. We made a pugh chart comparing widely adopted allergy testings with two other testing methods that we came up with.
Monday, February 3, 2014
Thoughts on Brainstorming
Hey everyone! I have been working on brainstorming ideas for the project and am stuck on creating some sort of saliva test strip. Since there are already test strips that test different things in saliva already, like pH, I was thinking we could create a comprehensive saliva test strip. Maybe we could combine each of those strips together so they can be tested for all on one strip. Another idea I had was to somehow modify an instrument that dental hygienists use when cleaning teeth, like the mirror; It is one of the only simple instruments I could think of that can be probably be physically modified somehow. Anybody have thoughts on this or other ideas?
- Lauren Kalfin
- Lauren Kalfin
Subscribe to:
Comments (Atom)